
总结内侧髌胫韧带(MPTL)的应用解剖及生物力学、重建技术及其临床疗效研究进展。
在中国知网、PubMed、Web of Science数据库中,检索2022年5月之前公开发表的关于MPTL解剖、生物力学及重建技术研究文献47篇;通过对上述文章的参考文献进行筛选,补充检索21篇。按照本研究纳入和排除标准,最终纳入47篇文献(中文文献5篇、英文文献42篇)进行分析和总结。
MPTL位于膝关节内侧支持带第二层,起自髌骨内侧下端。沿内下方走行,止于胫骨前内侧近端。MPTL内侧总约束力约为5%,并且主要在膝关节屈曲30°~90°的倾斜和旋转中发挥作用。此外,初次髌骨脱位常伴有内侧髌股韧带(MPFL)和MPTL的联合损伤。MPTL参与的重建方式主要分为单纯MPTL重建和MPFL联合MPTL重建,前者临床研究疗效良好,但单纯重建MPTL无法恢复内侧支持带原有的生物力学结构,故不推荐在临床中应用。在多项MPFL联合MPTL重建临床研究中,患者术后功能Lysholm评分、Kujala评分和国际膝关节文献委员会(IKDC)评分,以及髌骨高度、胫骨结节-滑车沟、髌骨外移度等影像学指标均得到有效改善,但MPFL联合MPTL重建手术适应证仍未达成共识。
对MPTL的应用解剖和生物力学研究进一步证实了MPTL在维持髌股关节稳定性中的重要作用,因此,MPFL与MPTL联合重建能恢复内侧支持带的解剖和生物力学。为了满足临床需要,尚需要进一步研究以论证该手术的适应证。


版权归中华医学会所有。
未经授权,不得转载、摘编本刊文章,不得使用本刊的版式设计。
除非特别声明,本刊刊出的所有文章不代表中华医学会和本刊编委会的观点。
外侧髌骨脱位是运动医学的常见疾病,约占膝关节损伤的2%~3%[1],尤其以青年女性常见。初次髌骨脱位若不伴有骨软骨骨折,一般仅需保守治疗;若存在骨软骨骨折或存在高位髌骨、股骨滑车发育不良、胫骨结节(tibial tuberosity,TT)-股骨滑车沟(torchlear groove,TG)间距(TT-TG)高值等解剖异常,则需要手术治疗[2]。然而,一项预测研究表明初次髌骨脱位经保守治疗复发率高达50%[3],而再脱位后常规需要外科手术干预。内侧支持带提供接近90%的抗外移稳定性,该稳定结构包括内侧髌股韧带(medial patellofemoral ligament,MPFL)、内侧股四头肌腱股韧带(medial quadriceps tendon femoral ligament,MQTFL)、内侧髌胫韧带(medial patellotibial ligament,MPTL)和内侧半月板韧带(medial patellomeniscal ligament,MPML)[4],其中MPFL在防止外侧脱位中起主要作用。因此,髌骨脱位的传统手术方案为MPFL重建术,但一项针对629例行MPFL重建手术患者的系统评价显示术后并发症率仍高达26.1%[5],包括髌骨骨折、术后髌骨不稳、屈曲障碍和膝前疼痛等。考虑到髌骨脱位后常伴有MPFL和MPTL的联合损伤[6],为解决这一问题,MPFL和MPTL联合重建术在国内外逐步展开研究,并且临床疗效显著[7, 8, 9, 10, 11, 12, 13, 14, 15]。目前,MPFL解剖学、生物力学以及重建技术已进行广泛研究,对MPTL也有一些基础研究,只是临床应用还较少。笔者以“内侧髌胫韧带”“解剖”“生物力学”“韧带重建”和“medial patellotibial ligament”“anatomy”“biomechanics”“ligament reconstruction”等为关键词,在中国知网、PubMed、Web of Science数据库中,检索2022年5月之前公开发表的关于MPTL应用解剖、生物力学和重建技术的研究文献47篇,并对上述文献的参考文献进行筛选后补录21篇,共计检索到68篇。文献的纳入标准:(1)研究方法可靠,质量水平高;(2)临床研究中病例数不少于10例;(3)尸体研究膝关节标本不少于5例。排除标准:(1)临床研究和生物力学研究在设计方面存在缺陷;(2)内容不相符的研究。按照上述标准,最终纳入47篇文献进行分析,包括5篇中文文献和42篇英文文献,重点对MPTL的应用解剖、生物力学、重建技术及其临床疗效进行综述,旨在为髌骨脱位的手术治疗提供新思路和理论指导。
Slocum等[16]于1974年首次提出,MPTL为膝关节内真正意义上的独立结构;尸体研究也证实了MPTL的存在,文献报道其出现率高达100%[6,17, 18, 19, 20, 21]。MPTL为薄层韧带,起自髌骨内侧下端,沿内下方走行,止于胫骨前内侧近端。膝关节内侧支持带可分为3层:第1层为深筋膜,第2层为内侧支持带浅层及前方结缔组织,第3层为内侧支持带深层及膝关节囊。许多学者认为,MPTL位于第2层[6,22]。MPTL胫骨侧附着点位于胫骨下方前内侧、胫骨关节线下方14~20 mm[5, 6];也有学者将其附着点精确在胫骨内侧结节,附着面积为46.3 mm2[19]。MPTL髌骨侧附着部位与MPML相同,均位于髌骨内侧远端1/3,附着面积为27.4 mm2,附着中心点位于髌腱附着点内侧缘内侧3.5 mm和近端3.5 mm,内侧缘距髌骨上级和髌骨下极的距离分别是31.2 mm和18.2 mm[19];另有研究显示,MPTL髌骨侧附着点距髌骨下极3.6 mm[6]。受个体因素影响,各家报道的MPTL长度及宽度值有些许差异,MPTL长度为44~55 mm、宽度为12~22 mm[6,19,21, 22]。其次,MPTL在走行过程中与髌腱形成18.5°±4.9°夹角[6]。
生物力学研究显示,MPFL是防止髌骨外侧脱位的主要稳定结构,其对髌股内侧约束力的贡献超过50%,而MPTL在内侧总约束力占比最小,约占5%[6,10,20,23, 24, 25]。Panagiotopoulos等[26],在膝关节屈曲30°时,测量逐层离断内侧支持带后髌骨外侧移位位置,结果显示MPTL对髌骨内侧稳定性贡献占比约13%。需要注意的是,逐层离断内侧支持带的顺序不同会产生不同的结果[27]。研究发现,膝关节屈曲0°~30°时,MPFL在髌骨外移、倾斜及旋转的贡献度分别为72%、76%及62%,而MPTL的贡献度分别为26%、28%及32%;膝关节屈曲30°~90°时,MPFL在这三种运动中贡献度分别降到52%、28%及0,而MPTL在这三种运动中贡献分别提升到46%、72%及92%[5]。这些结果表明,MPTL主要在膝关节屈曲30°~90°的倾斜和旋转中发挥作用[21,28],而MPFL在此时发挥的作用较弱。Hinckel等[6]研究显示,MPFL的刚度为(8.0±1.9)N/mm、形变为(19.3±8.2)mm、断裂时能量为(646.7±519.7)mJ、拉力为(72.0±32.5)N,MPTL的刚度为(17.0±8.5)N/mm、形变为(8.6±2.1)mm、断裂时能量为(865.6±635.5)mJ、拉力为(85.5±46.3)N。由此可见,与MPFL相比,MPTL显示出更高的刚度和更小的形变量,因此重建MPTL的材料也需具有更高的抗拉强度。
Ebied和El-Kholy[24]研究显示,在离断MPFL、保持MPTL完整时,膝关节屈曲0°~30°可发生外侧髌骨半脱位;当MPTL和MPFL同时离断时,膝关节屈曲0°~60°可发生完全脱位,修复MPFL后屈曲膝关节0°~10°仍可发生膝关节半脱位。这一结果表明,尽管MPTL抗外侧约束力的贡献占比较低,但其缺损后会导致髌骨外移增加。虽然髌骨外侧移位主要的约束结构是MPFL,但MPTL在维持髌骨内侧稳定性中仍然起重要作用[23,29]。
髌骨脱位时常伴发MPFL及MPTL的联合损伤,导致髌股关节运动力学发生变化,初次髌骨脱位仅通过保守治疗往往无法治愈;对于复发性或习惯性髌骨脱位,由于存在自身解剖异常因素,往往需要通过外科方式纠正解剖异常。因此,手术成为髌骨脱位治疗的主要方式。对单纯MPFL重建术,患者术后长期随访发现,有12%的患者存在客观或主观的髌骨不稳[5],这可能是重建后的MPFL松动或紧张度调节不当导致的。MPTL作为髌股关节的次级稳定结构,它在膝关节屈曲角度大于30°时,尤其是屈曲位的髌股关节稳定性方面起着重要作用[30]。研究显示,MPFL和MPTL联合重建能提高髌股关节稳定性和优化运动轨迹,使髌骨达到解剖复位[14]。Maffulli等[11]对34例复发性髌骨脱位患者采用MPFL与MPTL联合重建术治疗,术后平均随访3.1年,末次随访时患者改良Cincinnati评分从术前的(51±22)分增加到(90±19)分,Kujala评分从术前的(47±17)分增加到(82±17)分,并且所有患者在随访期间均未发生髌骨骨折、髌骨不稳等并发症。Yang和Zhang[15]采用MPFL与MPTL联合重建术治疗58例平均年龄22.6岁的伴有高位髌骨的髌骨脱位患者,术后随访2年,主观结果的优、良、一般、差率分别为87.9%、6.9%、3.4%和1.7%,Kujala评分、国际膝关节文献委员会评分明显升高,VAS评分则明显下降,全组仅1例患者在跑步过程中出现半脱位症状;影像学评估结果与功能评分类似,术后患者髌骨倾斜角、髌骨高度、髌骨外移度和TT-TG值均有明显改善。此外,后续研究也证实了该重建方法的疗效[13,28,31, 32]。由此可见,MPFL与MPTL联合重建术疗效值得肯定。临床上韧带损伤治疗方式分为急性损伤的韧带修复和陈旧损伤的韧带重建技术。目前,未查阅到MPTL急性损伤韧带修复相关报道,故下文主要对MPTL陈旧损伤韧带重建技术进行综述。
目前,针对MPTL重建的手术指征临床上并没有达成一致,在此我们根据现有研究总结出以下几点:(1)屈曲型不稳定,屈曲时发生髌骨习惯性脱位或侧向滑动。在膝关节屈曲30°~90°时,随着屈曲MPTL会逐渐收紧而发挥主要作用[21,33]。(2)存在复发危险因素的儿童(滑车发育不良、高位髌骨)。为避免增加骨性手术而损伤骺板,MPFL联合MPTL重建可以增加髌股关节的稳定性[34, 35]。(3)全身韧带松弛(存在膝关节过伸),增加额外的支持以改善单纯MPFL重建时约束力不足的情况[33, 34, 35, 36]。(4)随着膝关节旋转角增加而增加的膝关节旋转角度(Q角)、TT-TG和胫骨结节-后交叉韧带间距值分别为10°~15°、15~20 mm、21~24 mm时,膝关节屈曲运动中会使髌股关节和髌胫关节受力过载[37, 38, 39]。(5)轻微解剖异常(高位髌骨、股骨滑车发育不良和Q角增加):在不明确是否需要联合骨性手术时,或与MPFL重建联合骨性手术相比,联合MPTL重建的并发症更少时,优先选择该术式。
如选择髌腱为移植材料,仅需分离内侧1/3髌腱,保留其髌骨侧附着部位,游离胫骨侧后,向内移约1 cm处进行固定。固定方式是在胫骨侧作纵行长方形骨槽,与筋膜一起形成骨筋膜隧道,通过骨筋膜隧道或缝线锚钉固定内移后的髌腱,重建MPTL,见图2。Rillmann等[40]使用该术式治疗37例患者(41膝),术后仅1例出现反复半脱位,其余患者均获得良好疗效。国内蒋洪涛等[41]使用半腱肌为移植材料,对分别以缝线+锚钉固定重建MPTL与以可吸收挤压螺钉固定重建MPFL治疗的复发性髌骨脱位患者进行比较研究,发现后者疗效更好,而前者的膝关节功能恢复较差。
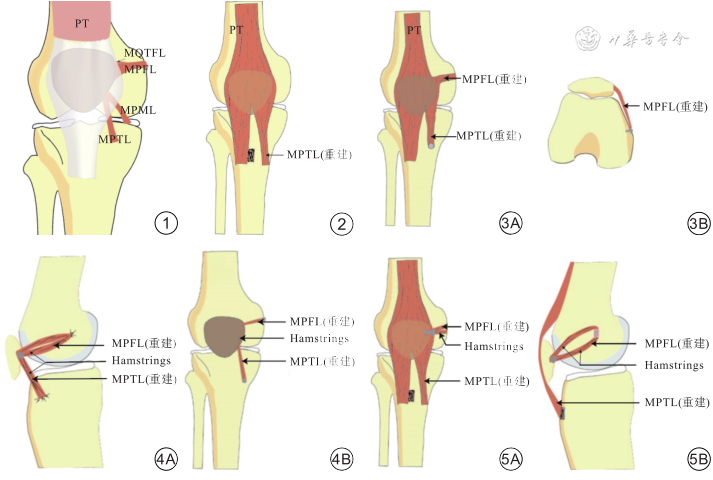
注:PT为髌腱;MPFL为内侧髌股韧带;MPTL为内侧髌胫韧带;MPML为内侧半月板韧带;MQTFL为内侧股四头肌腱股韧带;Hamstrings为腘绳肌
Hinckel等[12]使用髌腱进行MPFL联合MPTL重建时,在髌骨近端内侧分离宽约8 mm髌腱,保留其髌骨侧附着点,游离端用缝线锚钉固定在股骨内上髁与内侧收肌结节之间,此为重建的MPFL;后在髌骨远端取宽约6 mm的内侧髌腱,同样保留其髌骨侧附着点,将游离端用锚钉固定在胫骨关节面下方1.5~2.5 cm处,并且与髌腱所成角度保持在20°~25°,此为重建的MPTL,见图3。Hinckel等[12]应用上述方法治疗7例患者,术后平均随访5.5个月,其中1例出现伤口裂开,其余6例对术后结果均较满意。
Drez等[42]使用股薄肌或半腱肌进行MPFL联合MPTL重建时,髌骨侧使用缝线锚钉将肌腱附着在髌骨内缘侧上极下方1.5 cm处,胫骨侧则使用缝合固定于胫骨关节面下方1.5 cm处的骨膜,股骨侧缝合固定在收肌结节处,见图4A;也可保留股薄肌或半腱肌胫骨侧止点,髌骨内侧1/3由远端向近端钻直径4 mm或5 mm垂直骨道进行固定,股骨侧则用界面螺钉固定在MPFL解剖止点部位,见图4B。Drez等[42]应用上述方法治疗19例患者,15例术后接受随访的患者中有13例Fulkerson评分为优良,其滑车沟角和外侧髌股角也均较术前有所改善。
国内程松苗等[10]于2020年报道了其联合重建方法(图5):游离出内侧1/3的髌腱,保留其髌骨止点,通过骨筋膜隧道固定方式,将胫骨结节骨块植入胫骨平台内侧骨窗中,作为重建的MPTL;MPFL的重建则使用半腱肌作为移植物,需要在股骨内上髁和内收肌结节处钻取骨隧道,髌骨侧使用缝线和锚钉固定;对25例患者术后随访18个月,Kujala评分从术前平均54.6分改善至75.4分,Lysholm评分从术前平均43.5分改善至93.2分,术后的髌骨-股骨适配角、髌骨倾斜角和髌骨外移度(分别为4.1°、3.4°和7.4 mm)均较术前(分别为13.7°、16.9°和33.1 mm)显著改善,认为该术式在短期内取得良好的临床效果。
单纯MPTL重建和MPFL联合MPTL重建两种手术技术均在临床研究中获得认可;MPTL重建均使用自体肌腱进行移植,包括股薄肌、半腱肌、内侧髌腱及髂胫束,不同肌腱重建后疗效相当。最近一项针对单独MPTL重建和单独MPFL重建的生物力学对比研究显示,单独重建的MPTL在膝关节屈曲30°时无法抵抗髌骨的外侧约束力,故限制了其在临床中的应用[43]。Grantham等[14]对16例女性尸体标本膝关节的研究结果表明,MPFL联合MPTL重建才能最大限度地恢复髌骨在股骨滑车中原本的运动轨迹。然而,MPFL联合MPTL重建疗效是否优于传统的单独MPFL重建呢?这仍然还需更高等级的研究证据去验证,且对联合重建的适应证的完善是必不可少的。
联合重建术的主要优势:(1)对内侧支持带进行原有解剖结构重建,从而恢复原有髌股关节生物力学特点;(2)联合MPTL重建形成的约束力能减弱轻度的解剖异常对髌股关节稳定性的影响,从而避免联合的骨性手术(胫骨结节移位术、股骨滑车成形术等)对自身产生的不可逆危害[13,15,25];(3)MPTL的生物力学特性决定了其在膝关节屈曲时的重要性,因此,在屈曲型髌骨脱位中联合重建有不可逾越的优势[28]。
值得注意的问题:(1)MPTL与MPFL联合重建仅仅对韧带进行解剖重建,无法从根本上解决骨性发育异常问题,加之许多研究已经证实了MPFL联合骨性手术对伴有解剖异常的髌骨脱位患者的临床疗效[44, 45, 46, 47],联合重建MPTL反而会使手术方案复杂化;因此,若患者伴有严重的骨性解剖异常,例如重度股骨滑车发育不良、TT-TG高值等,仍应选择MPFL重建联合骨性手术(如股骨滑车成形术、胫骨结节移位术等)进行治疗。(2)在建立髌骨隧道时,隧道不易过大,以免引起髌骨骨折等并发症。(3)联合重建术需同时重建2个韧带,移植物固定后的张力需严格把控:在韧带固定前,应对膝关节屈曲过程中的髌骨轨迹的恢复情况进行判断,尤其是屈膝初始阶段,要保证膝关节在没有任何撞击和阻挡的情况下,顺利进入股骨滑车。
综上所述,由于MPFL是防止髌骨外移的主要稳定结构,目前髌骨脱位外科治疗仍以重建MPFL术式为主;然而,越来越多的尸体解剖及生物力学研究结果显示,MPTL也是维持髌骨稳定性的重要结构。目前对MPTL解剖和生物力学研究进一步证实了MPTL在维持髌股关节稳定性中的重要作用,MPFL与MPTL联合重建能恢复内侧支持带的解剖生物力学;而单独MPTL重建由于无法恢复髌骨原有的外侧约束力,故不推荐其在临床中应用。但是,对于MPFL与MPTL联合重建术的手术适应证,目前学术界尚未形成一致意见。为了满足临床需要,需要对单纯MPFL重建和MPFL联合MPTL重建进行前瞻性随机对照研究。另外,联合重建术式多种多样,将来需要通过比较研究或者探索新的手术方式,找出一种恢复解剖生物力学结构、手术创伤最小化的最佳手术方案。
所有作者声明不存在利益冲突

























