
食管切除和淋巴结清扫是食管癌治疗的基石,上纵隔淋巴结清扫对于食管癌精准分期和改善病人预后具有重要价值。左侧喉返神经旁淋巴结清扫是食管外科极具挑战的操作,其解剖边界和清扫范围尚无相关共识。近年来,随着腔镜技术尤其是机器人手术系统在食管切除术中的应用,上纵隔微解剖概念的引入,笔者团队提出左侧喉返神经旁淋巴结清扫边界,以实现精准、根治性、规范化清扫。笔者结合中心经验,对机器人手术系统辅助食管切除术左侧喉返神经旁淋巴结解剖边界、清扫范围和技巧进行深入阐述。


版权归中华医学会所有。
未经授权,不得转载、摘编本刊文章,不得使用本刊的版式设计。
除非特别声明,本刊刊出的所有文章不代表中华医学会和本刊编委会的观点。
食管癌是我国常见恶性肿瘤之一,病理学类型以鳞癌为主,食管癌切除术目前仍是食管鳞癌主要治疗手段[1]。与传统开放手术比较,微创食管癌切除术可降低术后并发症发生率,尤其是肺部并发症发生率,加快术后恢复,缩短住院时间,取得较满意的近期疗效以及与开放手术相似或更好的远期疗效[2, 3, 4, 5]。近年来,机器人手术系统逐步应用于食管鳞癌的外科治疗,其具有高清3D视角、360°旋转机械臂、有效过滤震颤等优势,可克服传统胸腔镜局限,在狭小空间易于完成高精度和高难度外科操作,尤其对于上纵隔左侧喉返神经旁淋巴结清扫较腔镜具有显著优势。左侧喉返神经旁淋巴结清扫是食管鳞癌切除术中的难点,目前国内外胸外科、食管外科或上消化道外科专家对食管鳞癌切除术中左侧喉返神经旁淋巴结清扫已达成共识,但对其解剖边界和清扫范围等尚无统一标准。笔者结合中心经验,对机器人手术系统辅助食管切除术左侧喉返神经旁淋巴结解剖边界、清扫范围和技巧进行深入阐述。
淋巴结转移和复发是影响食管鳞癌预后的重要因素,根治性淋巴结清扫可使术后分期更精准,降低局部复发率,改善病人生存[6]。双侧喉返神经淋巴结包括颈部气管食管沟(第101组)和胸腔双侧喉返神经链淋巴结(第106rec组)是食管鳞癌最常见转移部位,转移率高达20%~40%,清扫效能亦最高[7]。因此,双侧喉返神经淋巴结是食管鳞癌切除术中最重要的淋巴结清扫部位。
目前对于食管癌淋巴结清扫范围存有争议。在美国癌症联合会/国际抗癌联盟(AJCC/UICC)食管癌TNM分期系统中,N分期由阳性淋巴结数目决定,但对于淋巴结清扫范围未强制要求[8]。日本食管学会提出一种更精确但复杂的N分期系统,其中区域淋巴结根据不同的站点分为N1~N3水平,食管切除术中至少清扫二级站淋巴结(D2淋巴结清扫)[9]。2017年,Matsuda等[10]详细阐述食管鳞癌的淋巴结清扫方式:标准淋巴结清扫(腹上区和隆突以下的中下纵隔淋巴结清扫)、扩大纵隔淋巴结清扫(标准淋巴结清扫基础上行上纵隔及颈部气管食管沟淋巴结清扫)、3野淋巴结清扫(扩大纵隔淋巴结清扫的基础上行双侧锁骨上淋巴结清扫)。此外,有研究结果显示:补救性锁骨上淋巴结清扫对食管切除术后孤立性锁骨上淋巴结转移的病人亦可获得较好预后[11]。双侧喉返神经淋巴结因转移率高、清扫效能高,因此,包含双侧喉返神经在内的完全扩大纵隔淋巴结清扫术或3野淋巴结清扫术应成为食管鳞癌标准手术方式[10,12]。多项研究结果均显示:行上纵隔喉返神经淋巴结清扫术能显著改善食管鳞癌病人的无病生存和总体生存情况[13, 14, 15]。
由于存在肩胛骨、脊柱和腋窝结构,狭小肋间隙和狭窄上纵隔空间给胸外科医师施行微创食管癌切除术带来挑战。机器人手术系统可克服传统腔镜的局限性,更便于在狭小空间完成操作,机器人手术系统放大10倍的3D内窥镜视角使纵隔解剖可视化,机械臂的灵巧性为食管切除术中纵隔淋巴结清扫提供精细控制。目前多数研究结果显示:机器人手术系统较腔镜辅助食管癌切除术的优势是对纵隔淋巴结的清扫,尤其是空间狭小双侧喉返神经旁淋巴结清扫及对喉返神经的功能保护[16, 17, 18, 19, 20, 21]。2012年日本Suda等[16]比较16例行机器人手术系统和20例行腔镜食管癌切除术病人资料,其研究结果显示:机器人手术系统食管癌切除术能减少声带麻痹(P=0.018)和声音嘶哑(P=0.015)的发生率。2019年国内Chen等[17]的研究结果显示:与腔镜食管癌切除术比较,机器人手术系统能显著降低喉返神经损伤发生率(7%比17%,P=0.021)。2020年国内Yang等[18]通过倾向评分匹配分析机器人手术系统食管癌切除术(271例)和腔镜食管癌切除术(271例)的临床疗效,其研究结果显示:机器人手术系统食管癌切除术可提高喉返神经旁淋巴结清扫数目(4.8枚比4.1枚,P=0.012),但喉返神经损伤率高于腔镜手术(29.2%比15.1%,P<0.001)。短期随访结果显示:尽管两组病人总体生存和无病生存情况比较,差异均无统计学意义,但机器人手术系统病人纵隔淋巴结复发率更低(2.0%比5.3%,P=0.044)。这提示:机器人手术系统辅助食管癌切除术安全、可行,喉返神经旁淋巴结清扫更彻底,充分的纵隔淋巴结清扫可能降低局部淋巴结复发率。两项单中心回顾性研究结果显示:机器人手术系统食管癌切除术可获得更高的左侧喉返神经旁淋巴结清扫数目[19, 20]。最新一项Meta分析结果显示:机器人手术系统食管癌切除术可获得更满意的淋巴结清扫效果,且声音嘶哑的发生率明显降低(OR=0.624,95%CI为0.411~0.947,P=0.027)[21]。
笔者中心初期研究结果显示:机器人手术系统对上纵隔淋巴结清扫优于腔镜,对左侧喉返神经旁淋巴结清扫完成率优于腔镜,但两者喉返神经损伤率比较,差异无统计学意义[22]。笔者中心回顾性分析184例行食管癌切除术病人的临床资料(机器人手术系统组109例,腔镜组75例),其结果显示:度过学习曲线后,机器人手术系统组左侧喉返神经旁淋巴结清扫数目高于腔镜组[(5.4±2.7)枚比(4.4±2.2)枚,P=0.016],机器人组左侧喉返神经的损伤率为7.4%,腔镜组为22.5%[23]。上纵隔尤其双侧喉返神经旁淋巴结清扫是经胸食管切除术中极具挑战性的部分,胸腔镜在狭小空间的操作具有局限性,依靠胸腔镜对较深部位淋巴结清扫在技术上具有难度。传统食管癌切除术中腔镜器械精确解剖受限制,不合适的角度可能会在淋巴结清扫过程中损伤喉返神经,导致声带麻痹或由于器械限制使淋巴结清扫不充分。机器人手术系统具有高清3D视野、360°可旋转机械臂、过滤术者手部颤动等优点,使术者在淋巴结清扫过程中实现局部精准解剖,淋巴结精准清扫。
左侧喉返神经旁淋巴结清扫是食管鳞癌切除术中的难点。目前仅日本食管学会食管癌分期系统对喉返神经淋巴结进行了边界划定:上界为从锁骨下动脉上缘到胸骨上切迹,下界为喉返神经自迷走神经发出后向上弯曲的尾缘[24]。但这一标准对实际操作仍缺乏指导意义。
2015年Cuesta等[25]首先提出食管系膜概念,但未得到广泛接受。Tsunoda等[26]将系膜切除概念引入喉返神经旁解剖性淋巴结清扫,通过该方法,上纵隔淋巴结中位清扫数目为12枚,>Ⅱ级喉返神经麻痹发生率为11%。Fujiwara等[27]基于人类胚胎发育提出上纵隔外科解剖学“同心结构模型”假设。该模型包括内脏、血管和体壁层,3层结构由疏松的组织相连,构成外科切除平面。该模型的引入使喉返神经麻痹发生率从36.4%降至19.0%。Shirakawa等[28]提出内脏鞘和血管鞘的微解剖概念,内脏鞘包裹气管、食管和包含有喉返神经淋巴结的食管系膜,血管鞘包裹周围血管和神经,这两个鞘之间有一层薄膜,被认为是精准手术解剖平面。该微解剖概念的应用,使左侧喉返神经麻痹发生率从18.1%下降至8.7%,且极大缩短了机器人手术系统辅助食管癌切除术手术时间[29]。
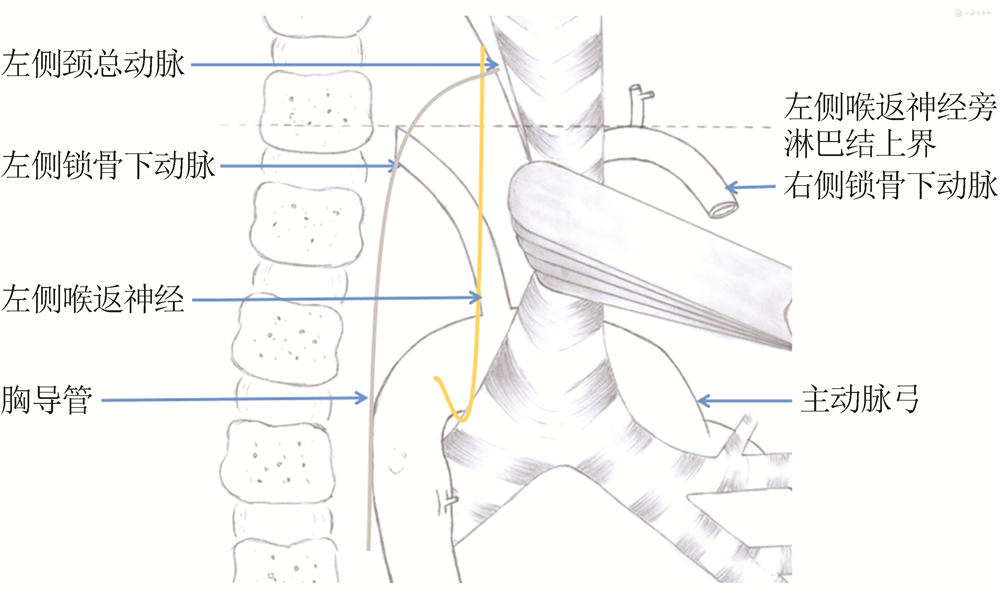
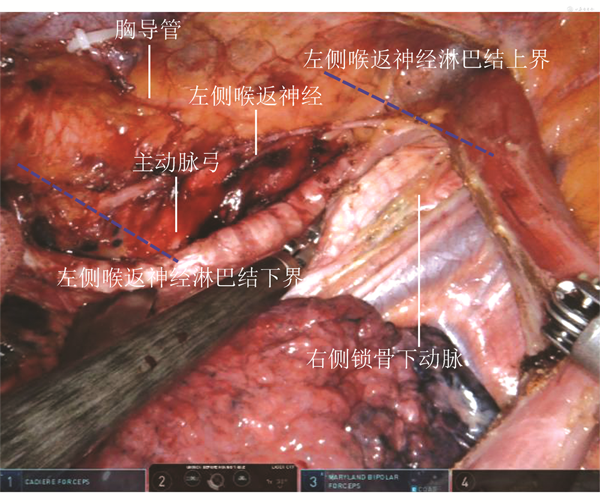
笔者团队结合机器人手术系统辅助食管癌切除及上纵隔淋巴结清扫经验,提出上纵隔左侧喉返神经旁淋巴结清扫边界:左侧喉返神经旁淋巴结是由左侧气管、食管,右侧主动脉及其分支、胸导管围成的包绕喉返神经的近似柱形区域内的淋巴结和软组织(图1,2)。左侧缘为内脏平面,由气管和食管组成,右侧缘为血管平面,由主动脉弓和左侧颈总动脉、左侧锁骨下动脉和胸导管组成,其间以疏松组织为界,构成外科操作平面;下界为主动脉弓下缘,喉返神经起始处,上界为右锁骨下动脉上缘和左侧颈总动脉、左侧锁骨下动脉交角构成的平面。解剖上,主动脉弓由右向左依次发出头臂干、左颈总动脉和左锁骨下动脉,头臂干发出右侧锁骨下动脉和右侧颈总动脉。双侧锁骨下动脉沿胸膜顶内侧,斜过前面达颈根部,在前斜角肌后方,弓形向外跨过第1肋骨移行为腋动脉。左侧锁骨下动脉直接发自主动脉弓,较右侧移行距离长。经右胸入路行食管切除术时,右侧锁骨下动脉便于解剖,其上缘易于识别和标记。而左侧锁骨下动脉直接发自主动脉弓斜向上自颈根部,移行距离长,经右胸入路行食管切除术时不易解剖和标记,以左侧锁骨下动脉上缘界定左侧喉返神经上界相对困难。将右侧锁骨下动脉上缘和左侧颈总动脉、左侧锁骨下动脉水平连线的平面作为左侧喉返神经旁淋巴结清扫上界更合适,便于解剖和术中标记。有学者提出以甲状腺下动脉作为喉返神经淋巴结清扫上边界,但笔者认为:甲状腺下动脉因甲状腺解剖变异存在差异,且甲状腺下动脉在解剖上不便于识别和定位。
笔者中心采用上述方法行规范的左侧喉返神经旁淋巴结清扫术,获得满意的淋巴结清扫效果和淋巴结清扫数目。笔者团队回顾性分析2017—2019年121例行机器人手术系统辅助食管癌切除术病人的临床病理资料,男100例,女21例;年龄为60岁(34~77岁)。手术时间为(320±43)min,术中出血量为(197±33)mL,淋巴结清扫数目为23枚(5~71枚)。121例病人中,74例左侧喉返神经旁淋巴结清扫数目为4枚(1~13枚),淋巴结转移率21.6%(16/74);101例右侧喉返神经旁淋巴结清扫数目为3枚(1~13枚),淋巴结转移率为18.8%(19/101)。术后总体并发症发生率为34.7%(42/121),包括声音嘶哑17例,肺炎13例,吻合口瘘9例,胸腔积液4例,切口感染2例,乳糜胸1例[30]。笔者团队2020年对113例病人行机器人手术系统McKeown食管癌切除术,其结果显示:左侧喉返神经旁淋巴结清扫率为89.3%,中位淋巴结清扫数目为4.08枚,淋巴结转移率为20%。
不同医疗中心采用机器臂的数量和打孔位置略有差异,主要依据主刀医师及助手的经验。笔者结合本中心经验,对机器人手术系统辅助食管切除术左侧喉返神经旁淋巴结清扫技术要点进行阐述。
机器人手术系统食管癌切除术手术步骤包括:经胸食管游离及淋巴结清扫;经腹胃游离、淋巴结清扫,管状胃制作;颈部食管胃吻合。(1)胸腔操作:病人取左侧90°卧位,机器人臂由病人背侧方向进入。采用3臂4孔法:右胸腋后线第6肋间置入机器人手术系统腔镜,右胸腋中线第3肋间及肩胛下角线第9肋间分别置入机器人1臂及2臂,腋中线第5或第7肋间作为辅助操作孔。建立人工CO2气胸,压力6~8 mmHg(1 mmHg=0.133 kPa)。首先于奇静脉弓上方打开纵隔胸膜,游离胸上段食管,保护右侧喉返神经及胸导管,并清扫上段食管旁、右侧喉返神经旁淋巴结;Hem-o-lok结扎并切断奇静脉弓,沿膜结构游离中下段食管至暴露膈肌裂孔,清扫膈上及中、下段食管旁淋巴结;采用牵引线将食管自辅助孔向前下方悬吊,助手采用肺挡压迫气管膜部,充分暴露左侧喉返神经区域,清扫左侧喉返神经旁淋巴结及软组织;最后清扫隆突下及双肺门淋巴结。(2)腹腔操作:病人取头高足低仰卧位,机器人臂由病人头侧方向进入。采用3臂5孔法:左侧脐旁2 cm处置入机器人手术系统腔镜,左侧腋前线肋缘下1 cm处及右侧锁骨中线脐上约6 cm处分别置入机器人1臂及2臂,右侧脐旁2 cm处及右侧腋前线处作辅助操作孔。建立人工CO2气腹,压力12~15 mmHg。超声刀沿胃大弯侧打开胃结肠韧带,保留胃网膜右血管弓;打开小网膜,解剖胃左血管,结扎并切断,清扫该区域淋巴结;游离近端胃及腹段食管,清扫贲门周围淋巴结,打开膈肌裂孔与胸腔相通。行上腹正中小切口,制作管状胃。(3)行左颈部胸锁乳突肌前缘斜形切口,暴露游离颈部食管,将管状胃自腹腔沿食管床拉至颈部,进行食管胃吻合。
左侧喉返神经旁淋巴结清扫是食管切除术中的难点,要做到根治性淋巴结清扫和神经功能保护(图3)。

1.左侧喉返神经旁淋巴结暴露:左侧卧位单腔气管插管(封堵器)与人工CO2气胸将肺彻底萎陷,采用肺挡将肺内残气彻底排出,进一步增加后纵隔暴露。充分游离全胸段食管,采用丝线牵引将食管经辅助孔牵引至前纵隔,采用肺挡压迫旋转法压迫气管膜部或气管左侧缘将气管向右侧旋转,充分暴露左侧喉返神经旁淋巴结区域(图3A)。
2.左侧喉返神经旁淋巴结气管侧游离:应用电钩自左主支气管处紧贴气管左侧缘将此处淋巴结连同周围组织分离(图3B),电钩自下而上沿气管左侧缘将左侧喉返神经旁淋巴结连同周围组织一并分离至左侧喉返神经上界(图3C)。此处助手尽量将气管向右侧顺时针旋转暴露,将气管左侧淋巴结及软组织一并分离(图3D)。
3.左侧喉返神经旁淋巴结血管侧游离:左侧喉返神经和软组织自气管侧游离后,主刀医师采用抓钳抓持纱布将左侧喉返神经旁淋巴结和软组织将背侧推送,电钩进一步分离至显露血管外膜。
4.采用旋转镂空法裸化左侧喉返神经:自左侧喉返神经上界水平,采用机器人手术系统分离钳(MALILAND钳)在分离的淋巴结和软组织间分离喉返神经,采用旋转镂空法彻底分离喉返神经周围淋巴结和软组织(图3E);自上而下采用同样方法,分离喉返神经周围淋巴结和软组织,直至分离至主动脉弓下水平,彻底裸化左侧喉返神经(图3F)。
5.避免喉返神经损伤:喉返神经直接断裂较少,喉返神经损伤通常是应用钳夹或能量器械导致的热损伤。抓钳钳夹淋巴结和软组织时,喉返神经分离后,直视下钳夹周围淋巴结和软组织;左侧喉返神经周围通常有伴行血管滋养喉返神经外膜,分离裸化喉返神经时损伤血管导致出血,采用纱布压迫法通常可有效止血;尽量避免应用超声刀等能量器械造成热损伤,如确需应用,需将此处淋巴结和软组织分离远离喉返神经。此外,部分淋巴结侵犯喉返神经时,需要分离钳和剪刀交替应用,将淋巴结自喉返神经剥离(图3G)。
6.整块切除左侧喉返神经旁淋巴结及软组织(图3H)。
食管切除和淋巴结清扫是食管癌治疗的基石,上纵隔淋巴结清扫对于食管鳞癌精准分期和改善病人预后具有重要价值[31]。精准清扫和保护喉返神经功能一直是食管外科不断追求的目标。近年来,随着腔镜技术尤其是机器人手术系统在食管切除中的应用,上纵隔微解剖的概念逐渐被熟识。笔者团队提出左侧喉返神经旁淋巴结清扫边界,实现精准、根治性、规范化清扫;同时对左侧喉返神经旁淋巴结清扫技术进行阐述,在清扫淋巴结时注意喉返神经的功能保护,可改善病人围术期生命质量。
所有作者均声明不存在利益冲突

























