
探讨新生儿Beckwith-Wiedemann综合征(Beckwith-Wiedemann syndrome,BWS)的临床表现和分子诊断经验。
回顾性分析复旦大学附属儿科医院新生儿科2016年1月至2020年12月收治的新生儿期诊断BWS患儿的临床资料,包括临床特征、分子诊断和是否合并其他先天疾病等。
共纳入16例BWS新生儿,男9例,女7例,胎龄34~39周,出生体重2 412~4 275 g。巨舌(9/16)和脐膨出(8/16)为主要临床特征,出生体重大于均值2个标准差(12/16)为最常见的次要特征。根据欧洲BWS诊断评分标准:评分≥4分的10例患儿为临床诊断BWS;5例评分≥2分但<4分和1例评分1分(其单绒毛膜双羊膜囊双胎评分为4分)的患儿为临床疑似BWS病例。13例进行分子诊断:临床诊断中6例和疑似病例中5例基因检测证实为印迹控制区2甲基化信号减低,临床诊断中2例为印迹控制区1甲基化信号增高。合并房间隔缺损、脑损伤各5例,合并甲状腺功能异常、脐带形态异常或脐血管异常各4例。
结合临床表现和分子诊断可在新生儿期及时发现并诊断BWS;BWS合并其他脏器异常比例高,确诊后有必要进行腹部超声、心脏超声、头颅MRI及甲状腺功能等检查。


版权归中华医学会所有。
未经授权,不得转载、摘编本刊文章,不得使用本刊的版式设计。
除非特别声明,本刊刊出的所有文章不代表中华医学会和本刊编委会的观点。
Beckwith-Wiedemann综合征(Beckwith-Wiedemann syndrome,BWS)是一种异质性过度生长综合征,由染色体11p15印迹区的功能调节异常引起[1, 2]。BWS患儿临床表现和严重程度复杂多样,临床表型包括巨舌、腹壁缺损、单侧过度增长和内脏肿大等[3, 4],在儿童期尤其2岁前罹患胚胎性肿瘤的几率约是正常儿童的600倍[5, 6],未经干预的患儿可能死于呼吸困难、进食困难、低血糖、电解质紊乱、肿瘤等。因此,及早诊治对BWS患儿至关重要。2018年欧洲科技合作协会赞助的欧洲先天性印记疾病网制定了有关BWS的诊断和评分专家共识[4],目前有关BWS患儿的研究主要集中在欧洲国家[7, 8, 9, 10, 11, 12, 13, 14, 15],针对亚洲人群的研究较少[16, 17, 18, 19],且国内对于新生儿BWS的报道多为个例报告。我院自2016年开始开展分子诊断,为进一步提高我国新生儿科医生对BWS的认识并规范诊疗,本研究对我院近5年收治的16例新生儿BWS进行回顾性分析。
选择2016年1月至2020年12月复旦大学附属儿科医院新生儿科诊断的BWS患儿为研究对象。纳入标准:(1)确诊BWS,2016—2018年根据主要临床表现进行诊断[3],2018年后参照BWS诊断和评分专家共识[4]进行诊断,并参照此共识对既往病例进行回顾;(2)足月儿入院日龄≤28 d,早产儿入院校正胎龄≤42周。本研究通过我院医学伦理委员会批准(2021-288)。
1.资料收集:本研究为回顾性研究,通过查阅电子病历收集患儿及其母亲信息,包括患儿性别、胎龄、出生体重、临床表现、实验室检查、治疗和预后、母亲围产期情况等。
2.BWS的临床特征与诊断[4]:每个主要特征2分,每个次要特征1分。(1)主要特征:巨舌、脐膨出、单侧过度增长、多灶和(或)双侧肾母细胞瘤或肾母细胞瘤病、高胰岛素血症(持续>1周,需要针对性的升糖药物治疗),病理示肾上腺皮质细胞肥大、胎盘间质发育不良或胰腺腺瘤病;(2)次要特征:出生体重大于均值2SD、面部单纯痣、羊水过多和(或)胎盘肥大、耳廓折痕和(或)凹陷、暂时性低血糖(持续<1周)、典型的BWS相关肿瘤(神经母细胞瘤、肾母细胞瘤、肝母细胞瘤、肾上腺皮质癌或嗜铬细胞瘤)、肾肿大和(或)肝肿大、脐疝和(或)腹直肌分离。
BWS诊断标准:(1)评分≥4分时临床诊断BWS且可不进行分子诊断;(2)评分≥2分建议行分子诊断明确是否为BWS;(3)评分<2分可不进行分子诊断;(4)分子诊断结果未见异常但评分≥2分,应请BWS专家进一步评估。
研究期间共收治26 082例新生儿,其中16例(0.06%)诊断BWS,男9例,女7例;双绒毛膜双胎1例(另1胎胎死宫内),单绒毛膜双胎1对;9例早产儿,7例足月儿;胎龄34~39周;出生体重2 412~4 275g;大于胎龄儿12例(12/16)。6例母孕期B超异常,其中5例为脐膨出,1例为频繁伸舌;脐带形态或脐血管异常4例,其中脐带水肿3例,5根脐血管1例;羊水过多1例。11例生后当天入院,其中8例因脐膨出入院,3例因早产且低出生体重入院;3例因低血糖在生后3 d内入院;2例在生后3周分别因低血糖和肝母细胞瘤入院。
1.主要特征:巨舌9例(9/16),脐膨出8例(8/16),单侧过度增长4例(4/16),高胰岛素血症3例(3/16)。见表1。
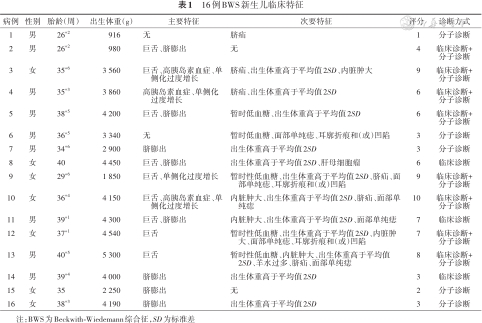
16例BWS新生儿临床特征
16例BWS新生儿临床特征
| 病例 | 性别 | 胎龄(周) | 出生体重(g) | 主要特征 | 次要特征 | 评分 | 诊断方式 |
|---|---|---|---|---|---|---|---|
| 1 | 男 | 26+2 | 916 | 无 | 脐疝 | 1 | 分子诊断 |
| 2 | 男 | 26+2 | 980 | 巨舌、脐膨出 | 无 | 4 | 临床诊断+分子诊断 |
| 3 | 女 | 35+6 | 3 560 | 巨舌、高胰岛素血症、单侧化过度增长 | 脐疝、出生体重高于平均值2SD、内脏肿大 | 9 | 临床诊断+分子诊断 |
| 4 | 男 | 35+3 | 3 860 | 高胰岛素血症、单侧化过度增长 | 脐疝、出生体重高于平均值2SD | 6 | 临床诊断+分子诊断 |
| 5 | 男 | 38+5 | 4 200 | 巨舌、脐膨出 | 暂时低血糖、出生体重高于平均值2SD | 6 | 临床诊断+分子诊断 |
| 6 | 男 | 36+5 | 3 340 | 无 | 暂时低血糖、面部单纯痣、耳廓折痕和(或)凹陷 | 3 | 分子诊断 |
| 7 | 男 | 34+6 | 2 900 | 脐膨出 | 出生体重高于平均值2SD | 3 | 分子诊断 |
| 8 | 女 | 40 | 4 450 | 巨舌、脐膨出 | 出生体重高于平均值2SD、肝母细胞瘤 | 6 | 临床诊断 |
| 9 | 女 | 29+6 | 1 850 | 巨舌、单侧化过度增长 | 暂时性低血糖、出生体重高于平均值2SD、脐疝、面部单纯痣、耳廓折痕和(或)凹陷 | 9 | 临床诊断+分子诊断 |
| 10 | 女 | 36+4 | 4 150 | 巨舌、高胰岛素血症、单侧化过度增长 | 内脏肿大、出生体重高于平均值2SD、脐疝、面部单纯痣 | 10 | 临床诊断+分子诊断 |
| 11 | 男 | 39+1 | 4 300 | 巨舌、脐膨出 | 内脏肿大、出生体重高于平均值2SD、面部单纯痣 | 7 | 临床诊断 |
| 12 | 女 | 37+1 | 4 540 | 巨舌 | 暂时性低血糖、出生体重高于平均值2SD、内脏肿大、面部单纯痣、耳廓折痕和(或)凹陷 | 7 | 临床诊断+分子诊断 |
| 13 | 男 | 40+5 | 5 300 | 巨舌 | 暂时性低血糖、内脏肿大、出生体重高于平均值2SD、羊水过多、脐疝、面部单纯痣 | 8 | 临床诊断+分子诊断 |
| 14 | 男 | 39+4 | 4 000 | 脐膨出 | 出生体重高于平均值2SD | 3 | 临床诊断 |
| 15 | 女 | 35 | 2 250 | 脐膨出 | 无 | 2 | 分子诊断 |
| 16 | 女 | 38+3 | 4 190 | 脐膨出 | 出生体重高于平均值2SD | 3 | 分子诊断 |
注:BWS为Beckwith-Wiedemann综合征,SD为标准差
2.次要特征:出生体重大于均值2SD 12例(12/16),暂时性低血糖5例,面部单纯痣6例,耳廓折痕和(或)凹陷3例,脐疝6例,内脏肿大5例,羊水过多1例,肝母细胞瘤1例。见表1。
3.评分结果:评分≥2分15例,其中评分≥4分的10例患儿为临床诊断病例,5例评分≥2但<4分的患儿为临床疑似病例;1例评分1分,为单绒毛膜双羊膜囊中的双胎之大,因双胎之小评分为4分归为临床疑似病例。见表1。
4.合并其他先天异常:合并房间隔缺损5例,隐睾2例,先天性喉软骨软化和颈部淋巴管瘤各1例。
13例患儿进行了基因组DNA甲基化特异性多重连接探针扩增技术检测,通过分子诊断明确为BWS;临床诊断中6例和临床疑似病例中5例基因检测证实为印迹控制区2甲基化信号减低,临床诊断中2例证实为印迹控制区1甲基化信号增高。3例因家属拒绝未行分子诊断,评分分别为3分、6分和7分。
1.甲状腺功能:所有患儿均进行甲状腺功能检测,12例正常;4例甲状腺功能低下,需口服左甲状腺素钠治疗,均为早产儿,其中1例基因检测明确为甲状腺分泌功能障碍5型的DUOXA2基因致病变异导致。
2.影像学结果:所有患儿均进行了腹部超声、心脏超声、头颅MRI检查,其中内脏肥大6例;房间隔缺损5例,脑损伤5例;2例消化道造影分别发现肠旋转不良和结肠冗长。
住院期间以对症支持治疗为主,包括呼吸支持、血糖维持、腹壁缺损修补术等,1例肝母细胞瘤患儿自动出院后失访,其余15例患儿均好转出院,出院时无呼吸困难、进食困难、低血糖等问题。
BWS是一种异质性过度生长综合征,由人类染色体11p15印迹区功能调节异常引起。BWS在活产婴儿中的发病率为1/15 000~1/10 000,约85.0%为无家族史的偶发病例[2],在辅助生殖婴儿中发病率高达1/1 100[20, 21, 22]。我院新生儿科近5年共收治16例BWS患儿,占所有收治新生儿的0.06%。
BWS患儿临床表现复杂多样,如产前超声提示巨舌、巨大儿、内脏肿大、羊水过多、胎盘肥大或胰腺过度生长、肾上腺囊肿或肿块等情况[23],则高度怀疑BWS,应选择有新生儿重症监护室的医院进行分娩。本研究中,5例母孕期B超提示脐膨出,1例提示频繁伸舌。Zhang等[24]分析了97例BWS患儿的临床表现,巨舌(83.2%)、腹壁缺损(71.3%)及耳廓折痕和(或)凹陷(55.3%)最为常见。本研究16例患儿中最常见表现为巨舌(9/16)和脐膨出(8/16),与既往报道一致;生后脐带形态或脐血管异常4例,包括脐带水肿3例和5根脐血管1例。新生儿单脐动脉[25]或4根脐血管[26, 27, 28]通常与先天发育畸形有关,脐带中5根或更多血管曾在连体婴和无脑儿中报道[29]。脐膨出是BWS的主要临床特征之一,但脐带异常尤其是脐血管异常与BWS的相关性有待进一步研究。2018年欧洲制定的BWS专家共识建议根据患儿的主要和次要临床特征进行评分,按照评分进行临床诊断并明确患儿是否需要进行分子诊断[4]。本研究16例患儿中15例评分≥2分需进行分子诊断,但3例家属拒绝;1例患儿评分虽为1分但因其双胎胞弟评分为4分且分子检测阳性,因此送检,结果亦为阳性。
由于未经干预的BWS患儿可能死于窒息、呼吸困难、进食困难、低血糖、电解质紊乱、肿瘤等疾病,因此,确诊后评估并制定合适的治疗方案非常重要。BWS患儿总体肿瘤发病率为8.0%,在儿童期尤其2岁前罹患胚胎性肿瘤的风险最高,最常见的肿瘤类型是威尔姆斯肿瘤(52.0%)和肝母细胞瘤(14.0%),其次是神经母细胞瘤(10.0%)、横纹肌肉瘤(5.0%)和肾上腺癌(3.0%)[30, 31, 32]。本研究中6例患儿进行了肿瘤指标检测,发现1例肝母细胞瘤。BWS患儿第1年生存率为90.9%[33],本研究16例患儿中15例经治疗好转出院,但尚未进行长期随访。除肿瘤高风险外,13%~20%的BWS患儿合并心脏发育畸形,明显高于正常儿童[9,12]。本研究中合并房间隔缺损5例,此外,合并脑损伤5例,合并肠旋转不良和结肠冗长各1例。因此,对BWS患儿进行脏器影像学检查和肿瘤指标随访非常重要。
本研究还发现4例患儿合并甲状腺功能异常,且1例基因检测明确为甲状腺分泌功能障碍5型的DUOXA2基因致病变异。目前仅少数报道提示BWS合并甲状腺功能低下[34, 35, 36, 37],2018年欧洲制定的BWS专家共识中并未建议在BWS患儿中常规随访甲状腺功能;虽然我国普遍对新生儿采集足跟血进行先天性甲状腺功能低下筛查,但有报道BWS患儿可在新生儿期之后出现甲状腺功能低下[36]。目前甲状腺功能低下与BWS的相关性尚不明确,是否需要对BWS患儿在新生儿期之后定期随访甲状腺功能有待进一步研究。
BWS临床表现复杂多样且严重程度差异大,早发现、早诊断、早干预并制定合适的治疗方案至关重要。本研究总结了16例新生儿BWS的病例资料,可为临床医生在新生儿期诊断BWS提供一定依据,但缺乏长期随访结果,未来需进行基于中国人群的BWS注册研究,为完善我国的BWS流行病学和遗传学特征并进一步提供相应的治疗方案和随访体系提供可能。
所有作者均声明不存在利益冲突


























本文中中文摘要中,结果部分“胎龄34~39周,出生体重2 412~4 275 g”应为“胎龄中位数(四分位数间距)36(34,39)周,出生体重中位数(四分位数间距)3 930(2 412,4 275)g”;正文中结果部分,“胎龄34~39周;出生体重2 412~4 275 g”应为“胎龄中位数(四分位数间距)36(34,39)周;出生体重中位数(四分位数间距)3 930(2 412,4 275)g”。英文摘要中,“with average gestational age of 34~39 weeks and average birth weight of 2 412~4 275 g”应为“with median (IQR) gestational age of 36 (34, 39) weeks and median (IQR) birth weight of 3 930 (2 412, 4 275)g”;“main clinical features”应为“most common cardinal features”;“common secondary feature”应为“major suggestive feature”;“confirmed to have reduced methylation signal in imprint control region 2”应为“identified with loss of methylation at imprinting control 2”;“had increased methylation signal in imprint control region 1”应为“were identified with gain of methylation at imprinting control 1”。更正的同时表示歉意!