Rosacea is a chronic inflammatory skin disease that primarily affects the centrofacial areas and mainly manifests as recurrent flushing and erythema. In recent years, there has been progress in the understanding of the diagnosis and treatment of rosacea. Therefore, a group of dermatological experts updated the guidelines based on the 2016 expert consensus statement on rosacea diagnosis and treatment in China. These new guidelines propose diagnostic criteria for rosacea at different sites to further standardize the diagnosis and treatment of rosacea in China.


Copyright © 2021 Hospital for Skin Diseases (Institute of Dermatology), Chinese Academy of Medical Sciences, and Chinese Medical Association, published by Wolters Kluwer, Inc.
This is an open access article distributed under the terms of the Creative Commons Attribution-Non Commercial-No Derivatives License 4.0 (CCBY-NC-ND), where it is permissible to download and share the work provided it is properly cited. The work cannot be changed in any way or used commercially without permission from the journal.
Rosacea is a chronic recurrent inflammatory disease that often occurs in the centrofacial areas and mainly involves the facial blood vessels, nerves, and hair follicular sebaceous units.1 According to the latest meta-analysis of epidemiological data in a large-scale population, the average prevalence rate of rosacea is 5.46%.2 A 2019 survey of 10,095 Changsha community residents showed a 3.48% prevalence rate of rosacea in the area,3 while a 2020 survey of 9227 college students from two Chinese universities showed a prevalence of 3%.4 Rosacea commonly presents as flushing, persistent erythema, papules, pustules, and telangiectasia, and usually affects women aged 20-50 years,5 but can also occur in children and older adults.6 To standardize the diagnosis and treatment of rosacea, the subprofessional dermatology committee of the Dermatology Branch of the Chinese Medical Doctor Association formulated the first version of the expert consensus on rosacea diagnosis and treatment in China in 2016. During the past 5 years, research on rosacea has made rapid progress, increasing the understanding of rosacea in China. Therefore, the Rosacea Research Center of the Chinese Society of Dermatology and the Rosacea Professional Committee of the Chinese Dermatologist Association organized relevant experts to formulate these updated guidelines based on the 2016 expert consensus and the latest local and international research, including evidence-based studies. These guidelines will aid dermatologists in their continued learning and practice.
Rosacea is generally considered to be a chronic inflammatory disease induced by multiple factors based on a genetic background of abnormal natural immunity and neurovascular regulation. The pathogenesis of rosacea mainly involves the following aspects discussed below.
Some patients with rosacea exhibit familial aggregation. Genetic and acquired environmental factors have led to disease development in twins, with each twin having half of the risk factors.7 The genes related to rosacea include HLA-DRA (such as DRB1*03:01, DRB1*02:01, and DQA1*05:01), BTNL2, PRELID2, and KCTD16.8
Neurovascular dysregulation is believed to play an important role in the pathogenesis of rosacea.9 Various external physical or chemical factors directly stimulate sensory neurons and promote the release of neuropeptides that activate transient receptor potential vanilloids 1-4 and transient receptor potential ankyrins (eg, TRPA1).10 These neuropeptides include substance P, calcitonin generelated peptide, and vasoactive intestinal peptide,10 which not only cause neurogenic inflammation but also induce vasoconstriction regulation disorders, leading to symptoms such as flushing and erythema. To a certain extent, mental factors, such as depression, anxiety,11 and type A personality,12 are involved in the occurrence and development of rosacea and are closely related to the mechanism of neurogenic inflammation.
Abnormal activation of the innate immune response plays an important role in the development of inflammation in rosacea. Rosacea lesions have significantly increased expressions of a variety of innate immune-related molecules, such as toll-like receptor 2 and antimicrobial peptides, and significantly increased numbers of many cell types, such as mast cells, macrophages, and neutrophils.13 Various external factors, such as ultraviolet radiation, pathogen colonization, and infection, promote the expression of antimicrobial peptides, such as leukocidins. These external factors also induce enhanced kallikrein kinaserelated peptidase 5 activity through toll-like receptor 2,14 vitamin D,15 and endoplasmic reticulum stress,16 and promote the transformation of the epidermal antimicrobial peptide cathelicidin into an activated interleukin-37 fragment17 that aggravates inflammation and induces angiogenesis, eventually causing rosacea.18,19
In rosacea, the water and sebum content of the stratum corneum in cheek lesions decrease, while transcutaneous water loss increases.20 The positive rate of lactic acid stimulation in rosacea skin lesions is significantly higher than that in normal controls, suggesting increased skin sensitivity.21 The expression of epidermal tight junction proteins, such as claudin 1 and claudins 3-5, is also significantly decreased.22 Skin barrier dysfunction in rosacea is mainly caused by inflammatory damage owing to the disease itself and the influence of environmental factors, such as inappropriate topical drugs, skin care products, and photoelectric therapy.
The presence of a large number of Demodex follicularis can play an important role in the pathogenesis of pimples, pustules, and granulomas in rosacea, with natural or acquired immunizations.23 However, although the reduction of Demodex folliculorum related to rosacea disease improvement,24 the clear cause of rosacea is still controversial. The pathogenesis of rosacea may also involve other microorganisms such as Propionibacterium acnes, Staphylococcus epidermidis, Malassezia species, Chlamydia pneumoniae,25 and Helicobacter pylori in the digestive tract.26
Rosacea predominantly affects the centrofacial convexities (most often the zygoma, cheeks, glabellae, chin, and nose), but can also affect the eyes and periocular region, and rarely, the outside areas of the face. Rosacea was formerly divided into four subtypes: erythematotelangiectatic, papulopustular, phymatous, and ocular.29 However, as different types of rosacea can coexist or transform, we suggest evaluating rosacea based on lesion areas.30 The clinical manifestations of rosacea are discussed below.
Flushing: Flushing lasts for several seconds to minutes, stimulated by neurovascular system triggers such as temperature changes, sun exposure, mood changes, and spicy stimulating food. Cheek flushing in rosacea is seen frequently, especially in China (99.6%), while nasal and perioral flushing are rare.31 Affected patients report paresthesia, such as burning and stinging sensations during flushing. Some patients with rosacea, especially those with dark skin, subjectively feel a burning sensation with no conspicuous erythema.
Persistent erythema: The most common manifestation of rosacea is persistent facial erythema or redness, with associated periodical aggravating or alleviating factors. This condition does not completely resolve spontaneously. All studied Chinese populations with rosacea have shown persistent erythema,31 thereby adding to its diagnostic ability. However, mild persistent erythema may be undetectable in darkskinned patients. To address this, the skin in front or behind the ears may be used as reference to better discern the lesions. Additional diagnostic examinations, such as dermoscopy, can be performed if necessary.
Papules and pustules: The typical symptoms of rosacea are dome-shaped erythematous papules, needle-sized superficial pustules, and nodularities.
Telangiectasia: Telangiectasia is typically imperceptible in dark-skinned patients. Dermoscopic examination can assist in the diagnosis.
Phymatous changes: Patients with rosacea present with thickened skin, glandular hyperplasia, and a globular appearance generally affecting the nasal area and other centrofacial convexities.
Sensitive skin symptoms: Patients with rosacea commonly have subjective symptoms, such as burning or stinging sensations, especially during paroxysmal flushing. Some patients experience tightness and itching, although these symptoms are generally mild.
Edema: Facial edema is a concomitant or secondary symptom of erythematous flecks, resulting from the increased permeability of capillary or lymphatic vessels and fluid extravasation caused by chronic inflammation. In some cases, inflammatory changes may cause pitting edema that lasts for several days. Patients with rosacea also present with solid (persistent and non-pitting) lymphedema. The two types of edema can occur simultaneously or independently.
Skin dryness: Most patients with rosacea present with skin dryness and an increased rate of water loss, while a few present with greasy skin.
Ocular manifestations: Ocular manifestations often affect the eyelids, eyelash follicles, and eyelid-related glands (ie, meibomian, sebaceous, and sweat glands). Approximately 31.3% of patients with rosacea have ocular involvement,3 including periocular papules, pustules, eyelid margin papules, pustules, telangiectasia, eyelid conjunctival hyperemia, local corneal stroma infiltration or ulcers, scleritis, and keratoscleritis. These patients present with a foreign body sensation, light sensitivity, blurred vision, and paresthesia (including sensations of burning, stinging, dryness, or itching).
A series of guidelines on the diagnosis and treatment of rosacea have been established in many countries, such as Canada, Switzerland, and the Netherlands.32 In 2002 and 2017, the National Rosacea Society assembled an expert committee to develop a standard and internationally accepted rosacea classification. The 2017 version proposed the following systematic diagnostic criteria: (1) the presence of one or both diagnostic cutaneous signs (ie, fixed centrofacial erythema in a characteristic pattern that may periodically intensify, and phymatous changes), and (2) the presence of two or more major features (eg, frequent and typically prolonged flushing, papules and pustules, telangiectasia, and ocular manifestations including eyelid margin telangiectasia, scleritis, sclerokeratitis, conjunctivitis, and keratitis).
The pathogenesis of rosacea is mainly considered to be centrofacial vascular manifestations. However, different facial areas (eg, cheeks, nose, and perioral area) manifest diverse signs. Based on the 2016 standard classification established in China, an expert committee proposed and developed a 2020 update that proposed diagnostic criteria for rosacea at different sites (Table 1). A diagnosis of rosacea is considered in the presence of one of the diagnostic signs in the cheeks, nose, and/or perioral area.
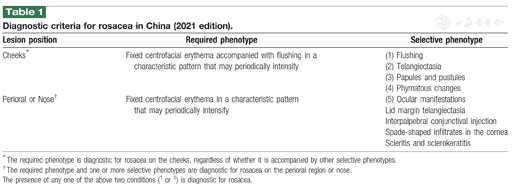
Diagnostic criteria for rosacea in China (2021 edition).
Diagnostic criteria for rosacea in China (2021 edition).
| Lesion position | Required phenotype | Selective phenotype |
|---|---|---|
| Cheeks* | Fixed centrofacial erythema accompanied with flushing in a characteristic pattern that may periodically intensify | (1) Flushing |
| (2) Telangiectasia | ||
| (3) Papules and pustules | ||
| (4) Phymatous changes | ||
| Perioral or Nose† | Fixed centrofacial erythema in a characteristic pattern that may periodically intensify | (5) Ocular manifestations |
| Lid margin telangiectasia | ||
| Interpalpebral conjunctival injection | ||
| Spade-shaped infiltrates in the cornea | ||
| Scleritis and sclerokeratitis |
* The required phenotype is diagnostic for rosacea on the cheeks, regardless of whether it is accompanied by other selective phenotypes.
† The required phenotype and one or more selective phenotypes are diagnostic for rosacea on the perioral region or nose.
The presence of any one of the above two conditions († or ‡) is diagnostic for rosacea.
The differential diagnoses include other conditions that also lead to frequent and typically prolonged flushing or persistent erythema, including the use of topical drugs (eg, glucocorticoids and retinoids), systemic drugs (eg, niacin and isotretinoin), topical chemotherapy, photoelectric therapy, menstrual or perimenopausal symptoms, and systemic diseases (eg, carcinoid syndrome, mastocytosis, and glandular medullary carcinoma).
The methods used to monitor rosacea are limited, and some are not specific for rosacea diagnosis. Thus, it is necessary to perform a comprehensive analysis in combination with the clinical features.
The typical diagnostic cutaneous signs of rosacea are a red or burgundy background with linear vessels arranged in horizontal and vertical lines to form polygons (polygonal vessels).33 The dermoscopic findings of papulopustular rosacea are tiny pustules centered on hair follicles with flushing. Granulomatous rosacea features structureless orange-yellowish papules. The use of dermatoscopy combined with clinical manifestations may facilitate faster diagnosis.
Reflectance confocal microscopic examination of rosacea lesions may reveal epidermal atrophy and varying degrees of flattening of spongy edema. Furthermore, there may be proliferation of spinous layer cells and an increase in the diameter of the sebaceous units of the hair follicles, with extensively dilated curled blood vessels. Some patients may have demodex mites in the sebaceous glands.
Although the pathologic changes in rosacea have poor specificity, they can aid in the diagnosis of rosacea and other differentials. Different rosacea lesions present with different histopathological signs.28 Telangiectasia and erythema in patients with rosacea usually comprise dilated vessels and lymphatics in the superficial dermis due to lymphocyte and plasma cell infiltration. Papules and pustules in rosacea have a marked infiltration of inflammatory cells (including lymphocytes, a few neutrophils, and plasmacytes) around the vessels and hair follicles. Hyperplastic and hypertrophic rosacea may present with hyperplasia of the sebaceous glands and fibrosis.
A computer-aided diagnostic system is a holistic and dynamic aid that provides an image of the facial vessel distribution and a dynamic evaluation of the severity of erythema and the therapeutic effect. This approach is easy and intuitive, with a better combination of clinical features.34
Persistent erythema in rosacea must be differentiated from that of facial eczema/atopic dermatitis, classic/photosensitive contact dermatitis, facial seborrheic dermatitis, hormone-dependent dermatitis, systemic lupus erythematosus, pemphigus erythematosus, and psoriasis. Papules and pustules in rosacea must be differentiated from those of acne vulgaris, eosinophilic pustular folliculitis, and lupus miliaris disseminatus faciei. Phymatous changes in rosacea must be differentiated from those of nasal sarcoidosis, skin neoplasms, and skin hyperplasia. Flushing in rosacea must be differentiated from that of carcinoid syndrome, menstrual or perimenopausal symptoms, and systemic mast cell hyperplasia. It is important to note that rosacea is often associated with acne vulgaris, seborrheic dermatitis, and facial eczema/atopic dermatitis.
The severity of rosacea is assessed based on different skin lesions. Various scales and evaluation methods have been used for the overall evaluation of rosacea, including the Flushing Assessment Tool,38 Global Flushing Severity Scale,39 Clinician's Erythema Assessment,40 Patient's Self-Assessment,41 and Investigator's Global Assessment.42 Scales used to assess the social psychological impact of rosacea include the Rosacea Quality of Life Index,34 Depression Anxiety Stress Scale,43 and Penn State Worry Questionnaire.44 Researchers in China have verified the effectiveness of the Rosacea Quality of Life Index in clinical practice.45 In 2019, the National Rosacea Society also proposed a monitoring tool for rosacea evaluation (Rosacea Tracker) that comprehensively evaluates and monitors the severity of rosacea based on skin lesions.46
The aims of rosacea treatment are to relieve or eliminate clinical symptoms, prevent recurrence, and improve patients’ quality of life. This proposed guideline classifies treatment methods in accordance with the level of evidence as A (one or more prospective randomized controlled clinical studies), B (larger prospective clinical studies with ≥20 subjects, but insufficient randomized control), C (small clinical studies with <20 subjects or retrospective studies), D (case series with ≥5cases), and E (individual case reports).47 The level of recommendation is classified as unanimously recommended, recommended, cautiously recommended, and not recommended.
Rosacea is a chronic and recurrent disease. Physicians should inform patients that symptoms can be substantially controlled or improved after 3 months of treatment, and that recurring episodes are likely to occur for several years or decades and require repeated intermittent treatment. However, drug treatment is generally not required if the patient only displays recurrent episodes of paroxysmal flushing, as these symptoms can be effectively controlled by scientific skincare, lifestyle modifications, and reduction of irritating factors.48 The common stimulating factors of rosacea include ultraviolet radiation exposure, emotional stress, high-intensity exercise, alcohol intake, hot and cold stimulation, spicy food, high or low environmental humidity, certain skincare products, low-quality sleep, and certain drugs.10 Patient education can help reduce the frequency of recurrent attacks in some patients.
Skincare is very important in preventing and treating rosacea. Patients should be instructed to take protective measures to prevent sunlight exposure, such as using parasols, sunglasses, and hats. Once the skin lesions are controlled, the patient may consider trying a simple and mainly inorganic sunscreen. Patients with rosacea should not wash their face with hot or cold water and should clean their face using a washcloth rather than their fingers. Patients should also minimize local facial massaging and friction, and avoid excessive cleaning.49 Patients should avoid the use of "three noes" skincare products (ie, products with no listed manufacturer or use-by date or quality certificate)50 and be cautious with the use of isolation cream and color makeup.51 When choosing skincare products, patients with rosacea should consult a doctor as much as possible for advice on choosing suitable low-irritant skincare products. A simplified skincare routine, including only external moisturizers, is recommended for patients with moderate to severe rosacea.
Skin barrier damage not only predisposes the patient to rosacea but also causes increased skin sensitivity. Therefore, skin barrier repair is the basic treatment for rosacea. After clinical verification, functional skincare products containing ceramide, hyaluronic acid, and calcium ions should be used to repair the skin barrier, relieve sensitive symptoms (such as dryness, tingling, and burning), and reduce clinical manifestations (such as paroxysmal flushing). The following products can be used for all types of rosacea.
Antimicrobial topical preparations: metronidazole, clindamycin, erythromycin, and ivermectin.
Metronidazole: Metronidazole kills demodex mites in hair follicles and has anti-inflammatory and antioxidant effects. Topical metronidazole has a therapeutic effect on papules, pustules, and erythema, but is not effective for vasodilation.52 The usual dose is 0.75% metronidazole in a cream/gel applied one to two times daily, which usually takes several weeks to take effect. Evidence level: A for papules and pustules; recommendation level: unanimous recommendation.
Clindamycin or erythromycin: Clindamycin is commonly used as a cream or gel with a concentration of 0.3% or 1%, while erythromycin is available as a cream with a concentration of 2%. Both drugs have a certain effect on papules and pustules, but have poor effects on erythema and telangiectasia. These drugs are used one to two times a day as second-line treatment for papules and pustules.53 Evidence level: A for papules and pustules; recommendation level: recommended.
Ivermectin: 1% ivermectin cream is a new drug for rosacea treatment that eliminates anti-follicular demodex mites.54 Ivermectin has a good effect on papules and pustules, but does not affect vasodilation. However, ivermectin cream is not available in the Chinese market and lacks relevant clinical data. Evidence level: A for papules and pustules; recommendation level: recommended.
Azelaic acid: Azelaic acid reduces the expression of kallikrein kinase-related peptidase 5 and antibacterial peptides, inhibits the release of cytokines induced by ultraviolet radiation, and improves rosacea papules and pustules.55 Azelaic acid is available in concentrations of 10%, 15%, or 20% in the form of a cream or gel, and is applied twice a day. Azelaic acid may initially cause itching, burning, and tingling, but these symptoms are generally mild and short-lived. However, azelaic acid is not available in the Chinese market and lacks relevant clinical data. Evidence level: A for papules and pustules; recommendation level: recommended.
Benzoyl peroxide: Benzoyl peroxide has antimicrobial effects and is used for the treatment of rosacea,56 but has some adverse reactions such as erythema, scaling, and local itching. Because of the increased skin sensitivity of patients with rosacea, benzoyl peroxide is only indicated for nasal or perioral papules and pustules. Evidence level: A for papules and pustules; recommendation level: cautiously recommended.
External vasoconstrictor drugs: Alpha-adrenergic receptor agonists, such as brimonidine, specifically act on the surrounding smooth muscles and constrict the facial blood vessels, reducing persistent erythema in the middle of the face. However, external vasoconstrictor drugs do not affect expanded capillaries, papules, and pustules. Currently, it is believed that external vasoconstrictor drugs may only temporarily suppress the erythema and do not effectively treat papules and pustules. A 0.5% brimonidine tartrate gel is commonly used once a day in countries other than China.57 Adverse reactions include increased rebound erythema/flushing, itching, and skin irritation. Considering the large differences in individual receptor levels and the different degrees of rebound, a risk assessment for brimonidine tartrate gel still needs to be performed in a large-sample study; thus, this gel should be used with caution in clinical practice. Another alphaadrenergic receptor agonist, oxymetazoline hydrochloride, constricts blood vessels by constricting the surrounding smooth muscle and exhibits an anti-inflammatory effect. In 2017, the US FDA approved 1% oxymetazoline hydrochloride cream for the treatment of persistent erythema in adults with rosacea.58 At present, these external vasoconstrictor drugs are not available in the Chinese market. Evidence level: A for erythema; recommendation level: cautiously recommended.
Salicylic acid: Salicylic acid has keratin-promoting, keratolytic, sterilizing, and antibacterial effects, and is effective for treating rosacea papules and pustules.59 Due to the differences in the effects and adverse reactions of different concentrations, salicylic acid must be used under the guidance of a doctor. Evidence level: B; recommendation level: cautiously recommended.
Antibiotic ointments or eye drops (eg, tetracycline and azithromycin) can be used for local eye treatment,60 while immunosuppressant eye drops (such as cyclosporine) can be administered if necessary.61 Demodex blepharitis requires anti-mite treatment,62 including topical metronidazole. When rosacea is complicated with dry eyes, artificial tears and anti-inflammatory treatments are required.63 Severe symptoms require referral to an ophthalmologist for diagnosis and treatment. Evidence level: none; recommendation level: unanimously recommended for artificial tears, recommended for cyclosporine eye drops, recommended for azithromycin eye drops, and recommended for tetracycline eye drops.
Antibiotics: Antibiotics are the first-line systemic treatment for rosacea papules and pustules.64 The US FDA approved the use of 40 mg/day doxycycline for the treatment of rosacea. Doxycycline at this dose has anti-inflammatory effects and minimizes flora imbalance and bacterial resistance, but has no antibacterial effects. A small number of patients may experience adverse gastrointestinal reactions, dizziness, and drowsiness. As there is no 40-mg form of doxycycline in China, it is recommended to use 50-100 mg doxycycline or 50-100 mg minocycline once a night for 8-12 weeks instead.65 For patients with rosacea who are younger than 8 years, intolerant of tetracycline antibiotics, or have other contraindications to doxycycline, macrolide antibiotics (such as 0.5 g clarithromycin once or twice a day or 0.25 g azithromycin once a day) may be used. Evidence level: A for papules, pustules, and erythema; recommendation level: unanimously recommended for papules and pustules, recommended for erythema.
Anti-anaerobic bacteria drugs: Metronidazole has anti-demodex and anti-inflammatory effects and is used as a second-line drug for rosacea.66 The usual metronidazole dose is 200 mg two to three times a day for approximately 4 weeks. Possible adverse reactions include gastrointestinal reactions, occasional headaches, insomnia, skin rash, and leukopenia. Evidence level: B for papules and pustules; recommendation level: recommended.
Isotretinoin contains anti-matrix metalloproteinases, inhibits inflammatory cytokines, and is used as first-line therapy for patients with hypertrophic rosacea and as a second-line option for papules and pustules when other treatments are ineffective.67 Isotretinoin is commonly used at doses of 10-20 mg/day68 for 12-16 weeks. Adverse reactions include dry skin and lips, erythema, and paroxysmal flushing; therefore, isotretinoin must be used in conjunction with moisturizers and lip balms. Clinicians must also be aware of the potential teratogenicity of isotretinoin and its impact on liver function and blood lipid levels. Isotretinoin cannot be used simultaneously with tetracycline. Evidence level: A for hyperplasia and hypertrophy, C for papules and pustules; recommendation level: unanimously recommended for hyperplasia and hypertrophy, recommended for papules and pustules.
Hydroxychloroquine has anti-inflammatory, anti-immune, and anti-ultraviolet radiation effects. Hydroxychloroquine inhibits the activation of mast cells induced by LL-37, reduces the release of inflammatory factors, and has a better effect on paroxysmal flushing or erythema than on papules and pustules.69,70 The dosage of hydroxychloroquine is 0.1-0.2g twice a day for 8-16 weeks, but the duration can be extended in accordance with the disease condition. If hydroxychloroquine is used continuously for more than 3-6 months, a fundus examination is recommended to rule out retinopathy. Evidence level: A for erythema, papules, and pustules; recommendation level: unanimously recommended for erythema, recommended for papules and pustules.
Carvedilol inhibits both α1-receptors and non-selective β-receptors, reducing the heart rate and nervousness of the patient. Carvedilol is mainly used for patients with intractable paroxysmal flushing and persistent erythema.71 The usual carvedilol dose is 3.125-6.25 mg one to three times a day for 6-28 months. Although these drugs are well-tolerated, it is necessary to monitor the heart rate and blood pressure for possible hypotension or bradycardia. Some patients experience a certain degree of rebound when the drug is stopped; therefore, the dose of the drug must be slowly reduced before the drug is gradually stopped. Evidence level: D for erythema; recommendation level: recommended.
Anxiolytics are suitable for patients with long-term mental stress and excessive anxiety. Antidepressants such as mirtazapine and paroxetine treat menopausal hot flashes by regulating vascular function,72,73 and exert anti-inflammatory effects through a variety of mechanisms.74 Therefore, anxiolytics are suitable for patients with rosacea with obvious symptoms, such as facial flushing, burning, and itching. Evidence level: none; recommendation level: cautiously recommended.
Appropriate photoelectric therapy can be applied to patients with rosacea in stable condition to improve inflammation and reduce telangiectasia and hypertrophic lesions. However, different operators have different opinions, and it is difficult to unify the operation parameters of phototherapy. Therefore, phototherapy should be used cautiously. In clinical practice, patients must be stable after a certain course of drug treatment before dermatologists can carry out treatments. As the use of different optoelectronic devices is closely related to the attending doctor’s experience, the following recommendation levels are based on usage by experienced doctors. In addition, frequent phototherapy should be avoided.
IPL therapy targets hemoglobin and sebaceous glands to reduce telangiectasia or hyperplasia, inhibit sebum secretion, induce anti-inflammation,75,76 and improve symptoms such as erythema and telangiectasia.77 IPL therapy is used to treat papulopustular rosacea; however, caution should be exercised in patients in the acute swelling stage. Evidence level: A for erythematous lesions and telangiectasia; recommendation level: recommended.
PDLs target hemoglobin to improve erythema and telangiectasia.78,79 PDL therapy is used in patients with phymatous rosacea to indirectly inhibit the formation and growth of vegetation by inhibiting angiogenesis.80 The clinical effect of sub-purpura-dose PDL therapy on erythema and telangiectasia is similar to that of IPL therapy.81 The main adverse reactions of PDLs are purpura and secondary pigmentation. Strategies used to minimize these adverse reactions include a good synchronous cooling system, prolongation of the pulse width, and selection of an appropriate therapeutic energy level.82,83 Evidence level: B for erythematous lesions and telangiectasia; recommendation level: recommended.
Carbon dioxide and erbium lasers target water, which is beneficial for removing skin hyperplasia tissue and softening scar tissue through gasification stripping, and is suitable for patients with mild to moderate phymatous rosacea.84 The main adverse reactions are scabbing, pigmentation after inflammation, and skin texture changes. Strategies used to minimize these adverse reactions include adopting the dot-matrix mode,85 narrowing the treatment area, and dividing the treatment into multiple sessions. Evidence level: E for phymatous lesions; recommendation level: recommended.
Nd YAG lasers target pigment, hemoglobin, and water tissues, producing a good therapeutic effect for papulopustular rosacea.86 Evidence level: B for papulopustular lesions; recommendation level: recommended.
LED therapy targets protoporphyrin IX and hemoglobin. Red light significantly improves inflammatory papules and pustules, while yellow light improves erythema and telangiectasia. LED therapy is recommended for patients with rosacea with obvious swelling and burns. Evidence level: E; recommendation level: recommended.
Based on the physical properties of the eddy current electric field, the RF repair therapy instrument uses the anti-inflammatory, dermal reconstruction, and antimicrobial effects of thermal energy to treat rosacea. A half-faced study of RF and PDL therapies showed that RF therapy was as effective as PDL therapy as a rosacea treatment.87 Some RF therapy instruments combined with restorative skincare products effectively improve dry skin symptoms, repair the skin barrier, and improve erythema. However, caution should be exercised in patients with rosacea with papules and pustules. For patients with rosacea in the swelling stage, RF repair may temporarily aggravate swelling; therefore, early communication with patients is necessary. Evidence level: C for erythematous lesions; recommendation level: recommended.
Only a few studies have reported the clinical efficacy of PDT. A limited number of studies have shown that PDT has a superior efficacy in patients with papulopustular rosacea than in patients with erythematotelangiectatic rosacea. PDT is a superior treatment option for papules and pustules in rosacea. In addition, PDT with PDL as the light source is superior to PDL alone in terms of short-term efficacy, but there are no differences between the two therapies in terms of long-term efficacy.88 The main adverse reaction of PDT is erythema. Evidence level: D; recommendation level: cautiously recommended.
Rosacea mainly characterized by telangiectasia or phymatous changes may be less responsive to drug treatments and may require appropriate surgical treatment.89,90
Surgical scratches and incisions are suitable for treating telangiectasia and small vegetative lesions. The length of the exposed blade of a threeor five-blade knife should be adjusted in accordance with the degree of nasal telangiectasia and hypertrophic local skin lesions. The nose is fixed with the index finger and thumb of the left hand, and the right hand is used to cut the nose skin with a knife in the shape of a cross. Each stroke is performed 10-15 times, with subsequent application of a gauze to stop the bleeding. The cutting is stopped once numerous filamentous papillae appear on the wound surface, giving a "redbayberry" appearance. The wound is then bandaged for 1 week after the operation. If the postoperative outcome is unsatisfactory, a second operation can be performed 3-6 months later.91 Evidence level: C for phymatous lesions; recommendation level: recommended.
For patients with single or multiple large vegetations, excision or excision is recommended. Before the operation, the operator should refer to the preoperative photos to roughly estimate the normal nasal morphology in accordance with the patient’s nostrils. The recommended methods are: (1) use of an electric knife or common scalpel to roughly remove the hyperplastic rhinoplasty, and then use of a cutting technique to repair the shape; (2) use of an electric knife or common scalpel to remove the isolated hyperplastic rhinoplasty before performing local suture treatment; (3) for patients with lesions with numerous large vegetations, the vegetations are first cut with an electric knife before shaping after hemostasis; and (4) skin grafting after resection.92 Evidence level: C for phymatous lesions; recommendation level: recommended. In recent years, some experts have used ultrasonic scalpels for resection and incision; this method has the advantages of fast cutting speed, good hemostasis, no overheating phenomenon, and no effect on the healing of incised tissue.93
Botulinum toxin type A (BTX-A) is a neurotoxic protein that reduces erythema and paroxysmal flushing in patients with rosacea by inhibiting the release of acetylcholine and neuropeptide from nerve endings. BTX-A also inhibits mast cell degranulation, thereby reducing inflammation.94 BTX-A is typically intradermally injected in the erythematous area at injection points spaced 1 cm apart and doses of 0.5-1.0 U. The main adverse reactions are slight pain and local congestion, which are generally self-limiting. Currently, there are no uniform standards for BTX-A in rosacea treatment. In addition, the duration of efficacy varies among patients. Generally, the length of treatment should be determined in accordance with the patient’s wishes and expectations. Evidence level: D for erythematous lesions; recommendation level: cautiously recommended.
Mild persistent erythema requires only skin barrier repair, protection against sunlight, and mood stabilization.
Moderate to severe persistent erythema is treated using oral antimicrobial drugs (such as doxycycline or minocycline) and hydroxychloroquine. The combined use of moisture-retaining skincare products that repair the skin barrier and 0.5% brimonidine tartrate gel is applied in severe cases; however, the erythema may initially be aggravated. Once the lesions are stabilized, IPL, PDL, or Nd YAG laser therapy can be considered to constrict the blood vessels and alleviate the erythema. RF repair treatment achieves good results and can also be used for erythema in patients with non-swelling rosacea. Red and yellow LED therapy is used to relieve swelling in patients with obvious swelling and a burning sensation.
For patients with moderate to severe erythema with obvious flushing and a strong burning sensation, carvedilol can be added. Patients with obvious anxiety, depression, and insomnia may require short-term antidepressant medication under the guidance of psychologists or psychiatrists. For patients who do not respond to local and systemic treatments, BTX-A may be injected in the erythematous area.
For mild lesions, metronidazole, azelaic acid, clindamycin, erythromycin, or ivermectin topical preparations can be used. The treatment effect is evaluated after 8-12 weeks. If a curative effect has been achieved, topical drugs are used as maintenance to achieve the desired effect. Otherwise, a combination of systemic antibiotics and/or hydroxychloroquine treatment may be considered.
For moderate and severe lesions, the first choice is oral doxycycline, minocycline, or combined oral hydroxy-chloroquine, while the second choice is oral clarithromycin, azithromycin, or metronidazole. If these drugs are ineffective after 4-8 weeks, clinicians should consider switching to oral isotretinoin, as it can be used in combination with external preparations.
IPL, PDL, or Nd YAG laser therapies are used to treat telangiectasia when the inflammation control of papules or erythema is relatively stable; however, the treatment may induce or aggravate the erythema, papules, or pustules.
Oral isotretinoin capsules are the recommended first-line treatment option. For patients with papules and pustules, oral clarithromycin and other antimicrobial drugs (such as topical metronidazole, azelaic acid, ivermectin cream, clindamycin, and erythromycin) can be taken simultaneously with other topical preparations. The treatment options for telangiectasia are PDL therapy, long-pulse-width Nd YAG laser therapy, IPL therapy, or surgical scratching. CO2 and erbium lasers or surgical ablation and resection are used to treat nodular hypertrophy.
For most patients with ocular symptoms, systemic treatment alleviates both the skin symptoms and the ocular symptoms. Systemic treatment can also be used in combination with cyclosporine eye drops, but is contra-indicated during the infection period. If there are dry-eye symptoms, high-quality artificial tears should be applied. Patients with meibomian gland-related corneal and conjunctival lesions should be referred to an ophthalmologist for appropriate treatment.
Drs. Heng Gu, Fei Hao, Wei He, Wei Lai, Wei Liu, and Hong-Fu Xie are Editorial Board Members of International Journal of Dermatology and Venereology. The article was subject to the journal’s standard procedures, with peer review handled independently of this editor and their research groups.

























